Provider Overview
Condition: Carpal tunnel syndrome (ICD-10: G56.00 unspecified, G56.01 right, G56.02 left)
Reference for OTs, hand surgeons, orthopedists, physiatrists, and other practitioners evaluating Svalboard for CTS management.
Primary Structures Affected
| Structure | Conventional Keyboard Loading | Svalboard Loading |
|---|---|---|
| Median nerve | Compressed at 30-65 mmHg; irritation from adjacent tendon swelling | Near-resting pressure (2-10 mmHg); reduced tendon volume |
| FDP tendons (x4) | High-amplitude, high-frequency excursion | Short excursion; force shifted to intrinsics |
| FDS tendons (x4) | PIP flexion per keystroke; adds tunnel volume | Low activation; tilt bypasses PIP flexion |
| FPL tendon | Active for thumb keys (spacebar, modifiers) | Reduced; thumb via low-excursion tilt |
| Transverse carpal ligament | Tensioned by wrist extension; compresses nerve | Relaxed in neutral; not tensioned |
Key Biomechanical Changes
| Parameter | Conventional Keyboard | Svalboard | Clinical Significance |
|---|---|---|---|
| Wrist posture | 20-30 deg extension | 0 deg (neutral) | Primary determinant of intracarpal pressure |
| Tendon excursion | Full FDP/FDS range per keystroke | Small (2-4 mm tilt travel) | Reduces cumulative friction and synovial irritation |
| Actuation force | 45-60 cN | ~20 cN (tunable to 8-10 cN) | Proportionally reduces tendon tension in tunnel |
| Primary movers | FDP, FDS (extrinsic, cross wrist) | Lumbricals, interossei (intrinsic, distal to tunnel) | Decouples finger input from carpal tunnel loading |
| Co-contraction | Continuous wrist extensor firing | None (hand supported) | Removes compressive load from stabilizer muscles |
| Forearm posture | Pronated | Neutral rotation | Reduces pronator teres compression of median nerve |
| Ulnar deviation | Common (reaching for lateral keys) | Eliminated | Reduces carpal bone displacement and tunnel deformation |
Muscle Shift: From Extrinsic to Intrinsic
From: FDP/FDS dominance (tendons transit the carpal tunnel)
To: Lumbricals and interossei (originate distal to the tunnel)
Neither intrinsic group sends contractile force through the tunnel. When they perform key activation, extrinsic flexors remain quiescent and tendon volume decreases.
Clinical Use Cases
Early / Mild CTS - Intermittent paresthesia; mild electrodiagnostic slowing, no axonal loss - Conservative management: splinting, activity modification, possible injection - Svalboard role: Reduces mechanical provocation during work; extends conservative window; concrete modification without work cessation
Post-Surgical Return to Work - After carpal tunnel release, returning to keyboard work at 4-8 weeks - Svalboard role: Reduces tendon loading in return-to-work progression; lowers recurrence risk; neutral posture protects healing site; supports graduated increase
Chronic RSI with Median Nerve Symptoms - Longstanding RSI with CTS component, possible comorbidities - Multiple failed conservative interventions - Svalboard role: Addresses biomechanical root cause; reduces upper extremity loading; compatible with concurrent treatments
Prescribing Considerations
- Learning curve: 2-4 weeks to basic proficiency, 2-4 months to approach prior typing speed from a standard keyboard
- Reduced speed during learning itself lowers cumulative loading
- No contraindications for CTS; neutral posture and low force are inherently conservative
- Compatible with night splints, anti-inflammatory protocols, and therapy programs
- Counsel patients: input device change, not a medical device; does not replace clinical treatment
The Clinical Problem
Carpal tunnel syndrome (CTS) is the most common compressive neuropathy of the upper extremity, affecting 3-6% of adults with ~10% lifetime prevalence in hand-intensive occupations. It is the largest contributor to RSI-related lost work-days in the United States.
Anatomy of the Carpal Tunnel
The carpal tunnel is a narrow, inextensible fibro-osseous canal at the base of the palm - rigid on three sides, semi-rigid on the fourth:
- Floor (dorsal): Carpal bones (scaphoid/trapezium radially; hamate/triquetrum ulnarly) form a concave cortical arch.
- Roof (volar): The transverse carpal ligament (flexor retinaculum) spans from the scaphoid tubercle and trapezium to the hook of the hamate and pisiform.
The walls cannot expand. Any increase in content volume elevates intracarpal pressure.
Contents of the Tunnel
Nine flexor tendons and one nerve pass through this space:
| Structure | Count | Function |
|---|---|---|
| Flexor Digitorum Profundus (FDP) | 4 tendons | DIP flexion of digits 2-5 |
| Flexor Digitorum Superficialis (FDS) | 4 tendons | PIP flexion of digits 2-5 |
| Flexor Pollicis Longus (FPL) | 1 tendon | IP flexion of the thumb |
| Median Nerve | 1 nerve | Sensory to thumb, index, middle, radial ring finger; motor to thenar muscles |
The median nerve lies just deep to the transverse carpal ligament and superficial to FDS, making it vulnerable to any volumetric increase.
Pathophysiology
Symptoms arise through a cascade:
- Increased intracarpal pressure - Resting pressure is ~2-10 mmHg. Wrist extension to 30 degrees raises this to 30-40 mmHg; combined extension and finger flexion can exceed 60 mmHg.
- Repetitive tendon gliding - Each keystroke drives FDP/FDS excursion through the tunnel, generating friction that provokes tenosynovial thickening and edema.
- Synovial hypertrophy - Chronic irritation causes fibrosis, further reducing available space.
- Sustained non-neutral posture - Prolonged extension tensions the transverse carpal ligament and displaces tunnel contents against rigid bony walls.
The result is median nerve compression:
- Paresthesia - numbness/tingling in thumb, index, middle, radial ring finger
- Pain - often nocturnal, radiating into the forearm
- Weakness - reduced grip and pinch strength
- Thenar atrophy - in advanced cases, wasting of APB, opponens pollicis, superficial FPB
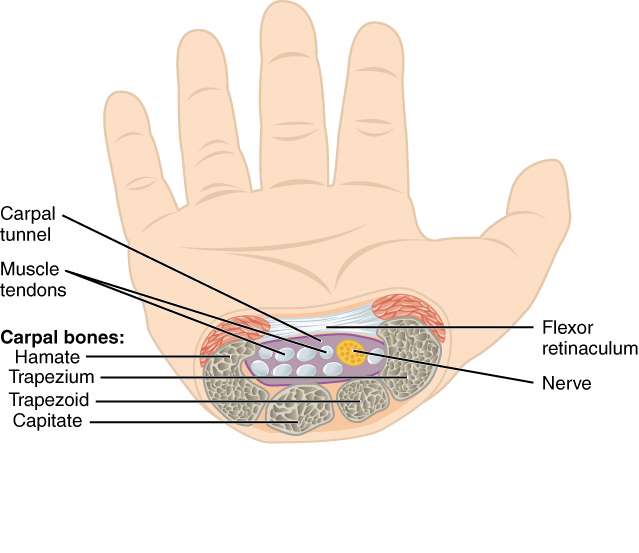
Axial cross-section of the carpal tunnel. Nine flexor tendons and the median nerve pass through this rigid fibro-osseous canal beneath the transverse carpal ligament (flexor retinaculum). Source: OpenStax Anatomy and Physiology, CC BY 3.0
Mechanical Drivers in Conventional Typing
Standard keyboards impose a biomechanical pattern that loads the carpal tunnel at every level.
High-Repetition Tendon Excursion
Every keystroke pulls FDP and FDS tendons through the carpal tunnel. At 60-80 WPM, that is ~18,000-24,000 total tendon excursions per hour across all digits. Each generates friction against the synovial sheath. This accumulates:
- Synovial irritation - fluid accumulation and inflammatory thickening
- Tenosynovial fibrosis - progressive over weeks and months
- Volumetric increase - compresses the median nerve in a fixed-volume space
Sustained Wrist Extension
Conventional keyboards force 20-30 degrees of wrist extension:
| Wrist Position | Intracarpal Pressure | Source |
|---|---|---|
| Neutral (0 degrees) | 2-10 mmHg | Werner & Armstrong, 1997 |
| 15 degrees extension | 18-24 mmHg | Keir et al., 1997 |
| 30 degrees extension | 30-42 mmHg | Rempel et al., 1997 |
| 30 degrees extension + finger flexion | 45-65 mmHg | Keir et al., 1998 |
Median nerve dysfunction threshold: 20-30 mmHg sustained. Standard typing routinely exceeds this.
Extrinsic Flexor Dependence
Key force (45-60 cN) is generated almost entirely by the extrinsic flexors - FDP and FDS - whose tendons cross the wrist through the carpal tunnel. Every unit of finger force requires tendon loading inside the tunnel.
Extensor Co-contraction
Wrist extensors (ECRL, ECRB, ECU) co-contract to stabilize the wrist in extension. This:
- Increases wrist joint compression
- Tightens the transverse carpal ligament
- Elevates intracarpal pressure
- Adds to fatigue and metabolic demand
Conventional Keyboard
- Wrist extended 20-30 degrees
- Full FDP/FDS excursion per keystroke
- 45-60 cN actuation force
- Sustained extensor co-contraction
- Pronated forearm
- Ulnar deviation common
- ~300-480 tendon excursions/minute
- Intracarpal pressure: 30-65 mmHg
Svalboard
- Wrist in neutral (0 degrees)
- Short tendon excursion
- ~20 cN activation force (tunable to 8-10 cN)
- No wrist stabilization required
- Neutral forearm rotation
- No ulnar deviation
- Reduced excursion frequency
- Predicted intracarpal pressure: near resting (~2-10 mmHg)
What Svalboard Changes
Svalboard alters which structures are loaded, how much, and in what posture.
1. Reduced Tendon Excursion
Keys activate via small-amplitude tilts (~2-4 mm), versus 3-4 mm travel plus full finger flexion arc on a conventional key. FDP/FDS glide distance drops accordingly.
- Less friction between tendons and synovial sheaths
- Less cumulative microtrauma per hour
- Reduced tenosynovial inflammation
- Lower volumetric swelling in the tunnel
2. Low Force Requirement
Far less actuation force than conventional switches, decreasing FDP/FDS contractile demand.
- Reduced tendon tension at the wrist
- Less compressive load through the tunnel
- Lower metabolic demand on extrinsic flexors
- Decreased fatigue-driven co-contraction
3. Neutral Wrist Posture
Each hand rests fully neutral - neither extended, flexed, nor deviated. Activations stay within the range that maintains this alignment.
Wrist posture is the largest modifiable risk factor for elevated intracarpal pressure. Moving from 30 degrees extension to neutral can reduce tunnel pressure by 30-50 mmHg during active use.
4. Palmar Support Removes Co-contraction
The hand rests in a supported cradle. Wrist extensors no longer fire to hold the hand above a keyboard, removing extensor co-contraction and its compressive load.
5. Shift Toward Intrinsic Muscles
Tilt-based input shifts primary movers from extrinsic flexors (FDP, FDS) to intrinsic muscles - the lumbricals and interossei.
- Lumbricals originate from FDP tendons in the palm, distal to the tunnel
- Interossei originate from metacarpal bones, entirely outside the tunnel
- Neither sends tendons through the carpal tunnel
- Their activation does not increase intracarpal pressure

Synovial sheaths of the flexor tendons at the wrist and hand. These sheaths line the carpal tunnel and facilitate tendon gliding - repeated friction within these constrained spaces drives the pathology of CTS. Source: Gray's Anatomy (1918), public domain
Clinical Impact
These changes converge on one objective: reduce mechanical load on the median nerve during sustained keyboard use.
Median Nerve Compression
Neutral posture returns intracarpal pressure to near-resting levels (2-10 mmHg), well below the 20-30 mmHg dysfunction threshold.
Tendon Irritation
Reduced excursion amplitude and frequency lowers cumulative tendon-sheath friction. Less friction, less tenosynovial inflammation, less volumetric encroachment.
Symptom Provocation
For many CTS patients, typing is the primary symptom trigger. Removing sustained extension and high-repetition tendon loading allows continued work without the pain-paresthesia cycle.
Co-contraction
Without extensor co-contraction, compressive load across the wrist drops, lowering baseline tunnel pressure independent of flexor tendon changes.
Conservative Management
For patients managed conservatively - splinting, activity modification, injection - Svalboard addresses the ongoing mechanical provocation these interventions do not. A night splint holds the wrist neutral during sleep. Svalboard extends that principle into 8 hours of typing without requiring work cessation.
Precedent: The Harrington Arthritis Research Center studied the DataHand (Svalboard's predecessor, same core design) and found a 71% reduction in pain after ~3 months of use (7.7 to 2.2 on a 0-10 scale) in keyboard users with existing pain conditions. The University of Arizona found 94% of users reported reduced wrist stress. See Supporting Evidence for details and caveats.
Effective Before and After Surgery
Svalboard is not a substitute for surgery when indicated. Severe CTS with thenar atrophy, persistent sensory loss, or axonal degeneration requires surgical decompression.
Surgery addresses only part of the problem.
What Surgery Does
Carpal tunnel release divides the transverse carpal ligament, expanding tunnel volume. Symptom relief rates: 75-90%.
What Surgery Does Not Do
Decompression does not reduce the mechanical workload:
- Tendon friction continues. FDP, FDS, and FPL still glide through the same space.
- Inflammation can recur. Chronic loading still provokes synovial thickening and scar tissue.
- Patients return to the same keyboards and the same loading pattern.
Recurrence: 3-12%, disproportionately in those returning to high-repetition hand-intensive work.
Before Surgery
For pre-surgical or conservatively managed patients:
- Removes sustained wrist extension
- Reduces tendon excursion volume and frequency
- Lowers intracarpal pressure during work
- Maintains productivity during conservative management
- May extend the window before surgery
After Surgery
For patients returning to work post-release:
- Less tendon friction in the post-surgical tunnel
- Lower demand on healing tissues
- Neutral posture avoids surgical site tension
- Reduces re-exposure to the precipitating biomechanical pattern
- Supports graduated return to full-time typing
User-Reported Outcomes
Users with pre- and post-surgical CTS report meaningful improvements:
- Pre-surgical: reduced daytime paresthesia, fewer nocturnal symptoms, better typing tolerance, and in some cases deferred surgery
- Post-surgical: smoother return to work, less symptom recurrence, reduced need for ergonomic accessories
These are user reports, not controlled evidence. They are consistent with biomechanical predictions of reduced carpal tunnel loading.
Clinical Summary: Carpal tunnel release expands the tunnel. Svalboard reduces the mechanical workload that drives tendon friction, inflammation, and elevated pressure. These are complementary. For patients who must keep typing - before or after surgery - reducing biomechanical load is a defensible strategy compatible with any standard treatment pathway.