Provider Overview
Condition: Dupuytren's contracture / palmar fascial fibromatosis (ICD-10: M72.0)
Focus: Adaptation, Not Treatment
Svalboard addresses the functional consequence of Dupuytren's - inability to type - without modifying the disease. If the digit cannot extend, eliminate the need for extension.
Key Biomechanical Change
Functional typing within restricted ROM. Key clusters activate with 1-2 mm displacement from resting position. A digit with fixed MCP/PIP flexion contracture retains sufficient ROM for the lateral and anterior micro-movements Svalboard requires.
Clinical Use Cases
-
Progressive Dupuytren's (Tubiana I-III) - continued keyboard function without waiting for intervention thresholds, without biomechanical stress on diseased fascia
-
Post-fasciectomy or aponeurotomy - earlier return to typing with reduced loading on healing tissue
-
Post-collagenase injection - typing without gripping or forceful extension during recovery
-
Patients deferring intervention - removes the main functional limitation without procedural intervention
-
Bilateral disease - split design with independent key clusters accommodates contracture in both hands
What to Expect
Patients typically adapt within 1-4 weeks. The 1-2 mm activation distance means even substantially contracted fingers retain sufficient ROM for all key activations. Patients report the affected digit is more functional on Svalboard than on any conventional input device.
Complementary to Standard Care
Svalboard integrates into existing treatment plans. It does not replace splinting, delay surgical referral, or interfere with rehabilitation. It removes typing from the clinical equation, letting treatment decisions focus on the contracture itself.
The Clinical Problem
Dupuytren's contracture is a fibroproliferative disorder of the palmar fascia. Thickening and shortening of fascial structures produce fixed flexion contractures, most commonly in the ring and small fingers.
Pathoanatomy
The disease originates in the palmar aponeurosis. Myofibroblast proliferation transforms normal fascia into pathological cords and nodules:
- Pretendinous bands contract into pretendinous cords, pulling the MCP joint into flexion
- Spiral cords form from the pretendinous band, spiral band, lateral digital sheet, and Grayson's ligament - displacing the neurovascular bundle centrally and superficially
- Natatory ligaments contract into natatory cords, limiting abduction and narrowing the web space
- Central cords extend past the MCP joint to involve the PIP joint - the most functionally limiting contracture
Clinical Presentation
- Nodules appear first in the distal palmar crease, firm and skin-adherent
- Cords develop over months to years as palpable longitudinal bands
- Contracture follows - MCP flexes first, then PIP
- Extension deficit is the hallmark
- Not primarily inflammatory, but repetitive fascial loading may accelerate progression
- Forceful grip and sustained extension become uncomfortable as contracture progresses
Functional Impact for Keyboard Users
The affected digit cannot reach the resting plane of a flat keyboard. Compensatory postures strain adjacent structures. As PIP contracture develops, the finger locks into a hook position - functional for grip, useless for conventional typing.
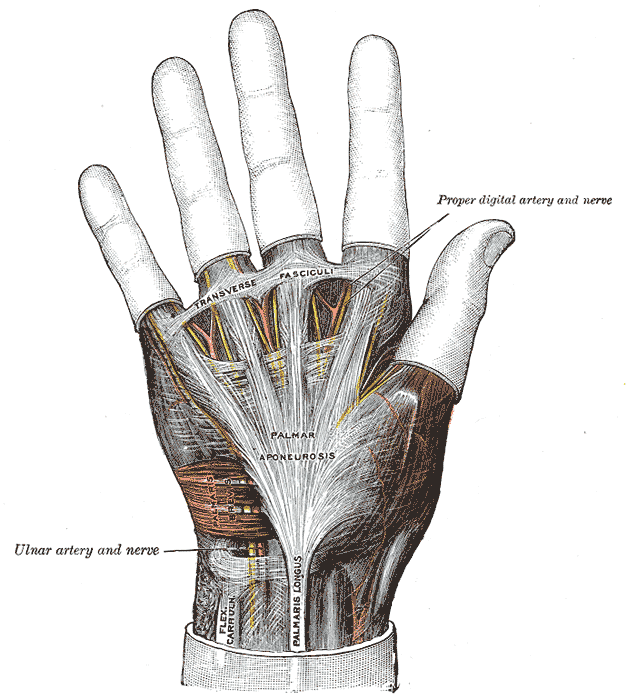
The palmar aponeurosis (palmar fascia). In Dupuytren's contracture, fibrotic nodules and cords develop within this fascial layer, progressively drawing the fingers - typically the ring and small finger - into flexion contracture. Source: Gray's Anatomy (1918), public domain
Mechanical Issue in Conventional Typing
Standard keyboards demand a biomechanical profile that conflicts with Dupuytren's:
- Repetitive full extension - every keystroke loads the shortened fascia against its mechanical limit
- Large motion arcs - 3-4mm travel plus inter-key reach requires full flexion-extension range
- Sustained extension posture - home row hover demands active extension a contracted digit cannot achieve
- Force through restricted ROM - altered force vectors generate abnormal shear across the palmar fascia
- Compensatory overload - adjacent digits and wrist absorb workload from degraded fingers
Repetitive fascial loading in a hand with active fibroproliferation may accelerate cord maturation. The goal: minimize fascial strain while preserving function.
Conventional Keyboard
- Full finger extension required for home row hover
- 3-4mm key travel per keystroke
- Large inter-key reach distances
- Contracted digit cannot reach keys without wrist compensation
- Repetitive extension loads shortened fascial cords
- Adjacent fingers compensate for restricted digit
- Grip-like posture for wrist stabilization strains palmar fascia
Svalboard
- No extension beyond resting position required
- 1-2 mm key activation travel
- Keys are immediately adjacent - no reaching
- Operates within the available ROM of a contracted digit
- Low fascial loading per keystroke
- Each digit works independently in its own key cluster
- Hand rests in supported neutral posture - no grip, no hover
What Svalboard Changes
Svalboard does not reverse fibrosis, dissolve cords, or restore extension. It sidesteps the biomechanical demands a contracted hand cannot meet and works within available ROM.
Reduced Movement Amplitude
Conventional typing demands 15-25mm of finger excursion per keystroke cycle. Svalboard keys activate with 1-2 mm of displacement. For a digit with 30 degrees of PIP contracture, this is the difference between impossible and trivial.
Operation Within Limited ROM
A finger locked at 30-60 degrees MCP flexion and 20-40 degrees PIP flexion still produces small lateral, anterior, and posterior movements from rest. Svalboard's key clusters use exactly these micro-movements. The contracted digit activates keys from wherever its resting posture places it.
Lower Force Requirements
Svalboard keys activate at a fraction of the force of mechanical switches. Over thousands of keystrokes per hour, this substantially reduces cumulative fascial strain.
Independent Digit Operation
Each finger operates its own key cluster. A contracted ring finger does not compromise adjacent digits - there is no shared surface to reach across.
Reduced Fascial Strain
Low travel (1-2 mm), low force, supported resting posture, and no extension requirement mean the palmar fascia is effectively unloaded during typing.
Clinical Impact
1-2 mm key travel replaces multi-centimeter finger excursion
Near-zero tensile load on palmar aponeurosis during typing
Productive input continues despite progressive contracture
No extension beyond resting position required
Clinical Summary
Svalboard preserves function through biomechanical adaptation. As contracture progresses, conventional typing becomes impossible for affected digits. Svalboard sidesteps this by removing the demands the contracture restricts.
Relevant across the disease spectrum:
- Early disease (nodules, mild contracture) - reduces repetitive fascial loading that may accelerate cord maturation
- Moderate disease (30-60 degree MCP contracture) - enables continued typing when conventional keyboards fail
- Severe disease (MCP + PIP contracture) - sufficient micro-movement remains to operate a key cluster
- Post-intervention (fasciectomy, needle aponeurotomy, collagenase) - typing resumes with reduced demand on healing tissue
Adaptation, Not Treatment Svalboard does not slow progression, reverse fibrosis, or restore ROM. It enables productive typing within the biomechanical constraints of the disease. Treatment decisions - observation, splinting, collagenase, aponeurotomy, fasciectomy - should proceed independently. Svalboard complements these interventions.